Redesign of the wayfinding system for an Opthalmology Hospital (2018)
Co-designed with: Tigmanshu Bhatnagar and Vikas Upadhyay
Client: R. P. Centre for Opthalmic Sciences, All India Institute of Medical Sciences, New Delhi India
Funded by: Indian Institute of Technology Delhi
Role: Field research, design, execution, testing and validation

The Rajendra Prasad Centre for Opthalmic Sciences has been pioneering in research, education and treatment of opthalmic conditions, for over 50 years. Their success in treating eye-related conditions helps them amass over 2000 patients in the out-patient department everyday, despite the entire centre having been designed in 1967 for a maximum capacity of 2000 persons. Thus ensues chaos during OPD times, as anxious patients and their carers negotiate a path to the correct OPD room for a check-up. The narrow corridors and poor information systems aggravate the situation, leaving security officers to double-up as information booths while trying to maintain order.
The Assistech Lab at IIT Delhi has been working in the assitive technology sector for over 20 years. They were invited to suggest solutions for the overcrowding of the Centre as well as improving information and navigation systems for the visitors of the centre. This project was divided into two phases, the first phase exploring physical information system interventions, and the second phase exploring digital interventions. This documentation is of the first phase, the second phase is available on Inclunav Maps and Inclunav Routes.
The team involved in this project included Tigmanshu Bhatnagar and I as consultants and project lead along with Vikas Upadhyay (research scholar, IIT Delhi) and three Masters students from the Department of Design. The project involved a study of the existing information systems through ethnographic and action research, development of new design solutions, and implementation of the solutions at the Centre along with feedback from the Centre staff. The solutions from both phases of the project continue to be in use at the Centre.
Research
Research into the existing state of the information systems involved journey-mapping and undergoing an eye check-up through the out-patient department on a day with high footfall. This method of action research allowed us to understand the emotional and physical requirements of the process for a patient to complete the most common journey through the Centre.
It was observed that for a physically fit, literate young male with good vision it typically takes 3.5 hours from getting in queue to book an appointment until exiting the Centre after an appointment. The waiting period comprises of 3 hours, while the check-up itself takes about 15 minutes per patient. Much of the waiting involves standing in queue or waiting outside the clinic, with limited seating facilities and in harsh weather for most of the year in New Delhi. Furthermore, most of the patients are already in discomfort due to an underlining condition for which they have come to the centre.

The journey itself involved navigating through long serpentine queues, often congested enough to confuse the patient of their intended destination. The Centre itself is air-conditioned, so the jostle becomes intense as one approaches the entrance of the Centre, nudging the person in front to try and cross the threshold as quickly as possible. The signages were far from useful, and often illegible for the average sighted individual. There was no hierarchy of information, and no information pertaining to persons standing in queue for registration. The helpdesk on one side of the entrance went unnoticed in the sea of anxious patients clambering into the centre, desperate for the comfort of an air-conditioned environment. The semblance of order came from the barriers in place and the security guards enforcing the queue systems.

To further understand the constraints of design interventions, we surveyed the space after working hours, noting key elements that contributed to the limited information access for visitors. We interviewed the security staff, the clinical staff and the cleaning staff for their understanding of the problems. We also studied the CCTV footage of the interiors to observe particularly crowded junctions, and the flow of patients through various periods of the out-patient clinic.

Based on our research we found three specific requirements of change which could improve wayfinding information for visitors to the centre. 1. Signages had to be made more legible, particularly at peak traffic hours. 2. Signages had to be placed as per the information required by the visitor at specific places in the centre. 3. An information hierarchy had to be established based on use of the space, requirements of the visitor and the constraints of the space.
Design and development
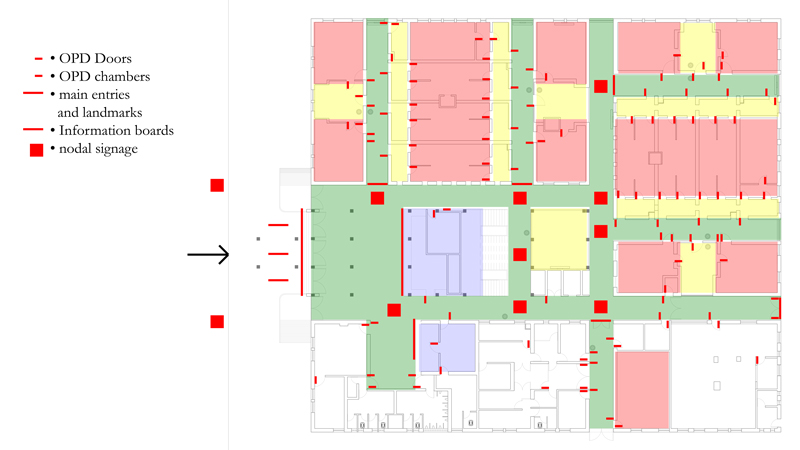
The first phase of ideation involved mapping of the spaces and the signages required at various points. We photographed the existing signages and their spaces, and then mapped the positions of the signages on a floorplan of the centre. Then we conceptualized how information access can be improved and created a new layout of the signages in the floorplan.
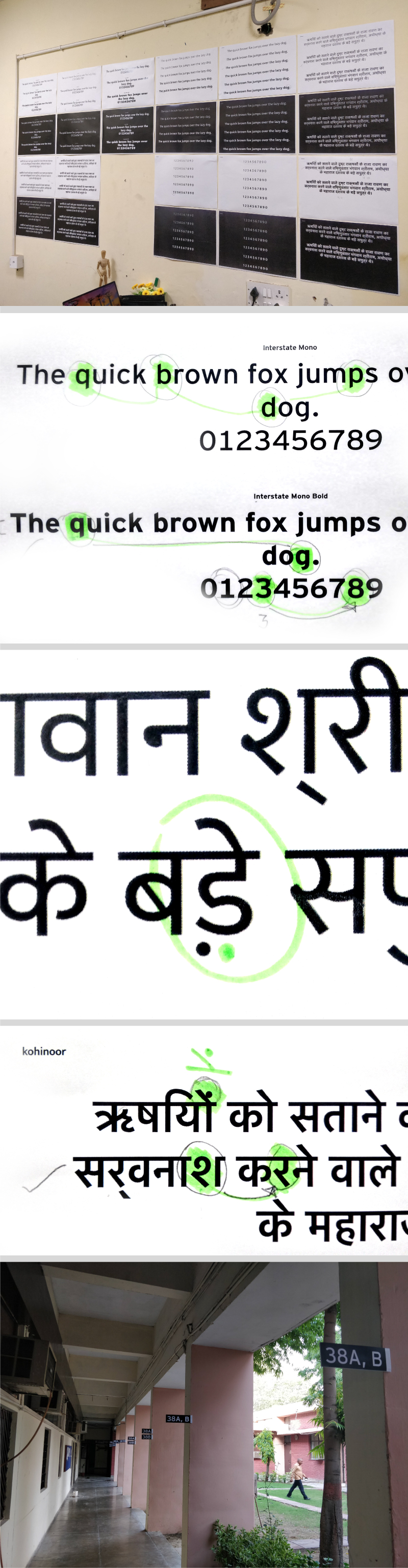
The language requirements, as discussed with the hospital staff indicated a predominant use of English and Hindi. We explored various typefaces that supported latin and devanagari fonts, and compared the glyphs to identify a suitable typeface to use for the signages.
A few signages were developed and tested at iit Delhi for colour contrast ratios and legibility over distances. The signages were also complemented with designs of icons that would reinforce the text, and provide navigational cues for the visitors.
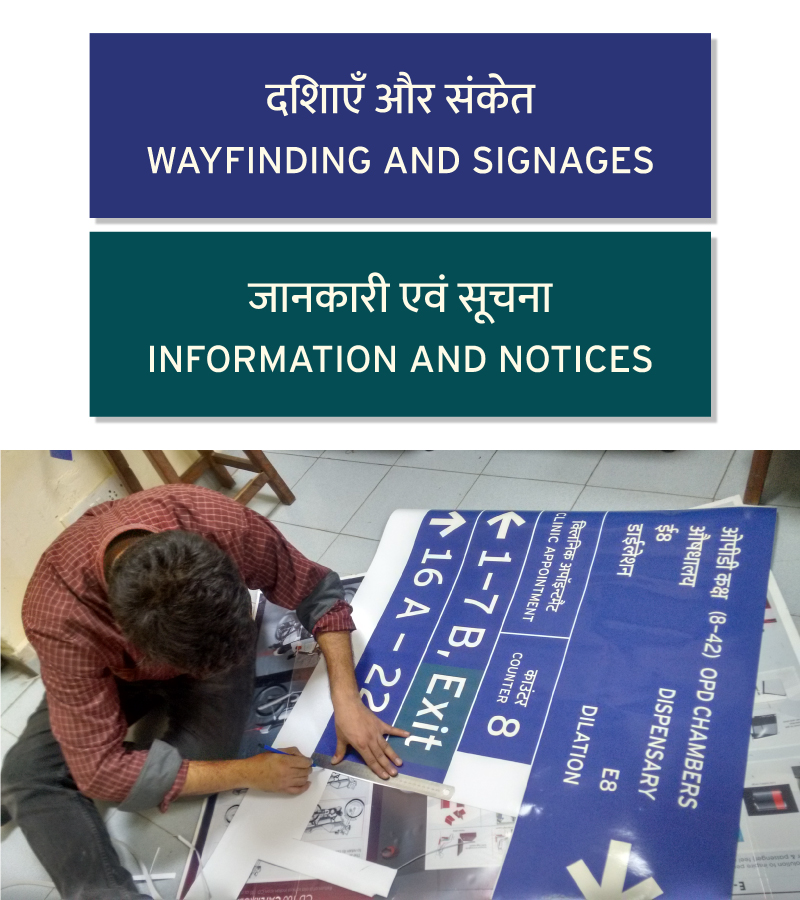
Prototyping and testing
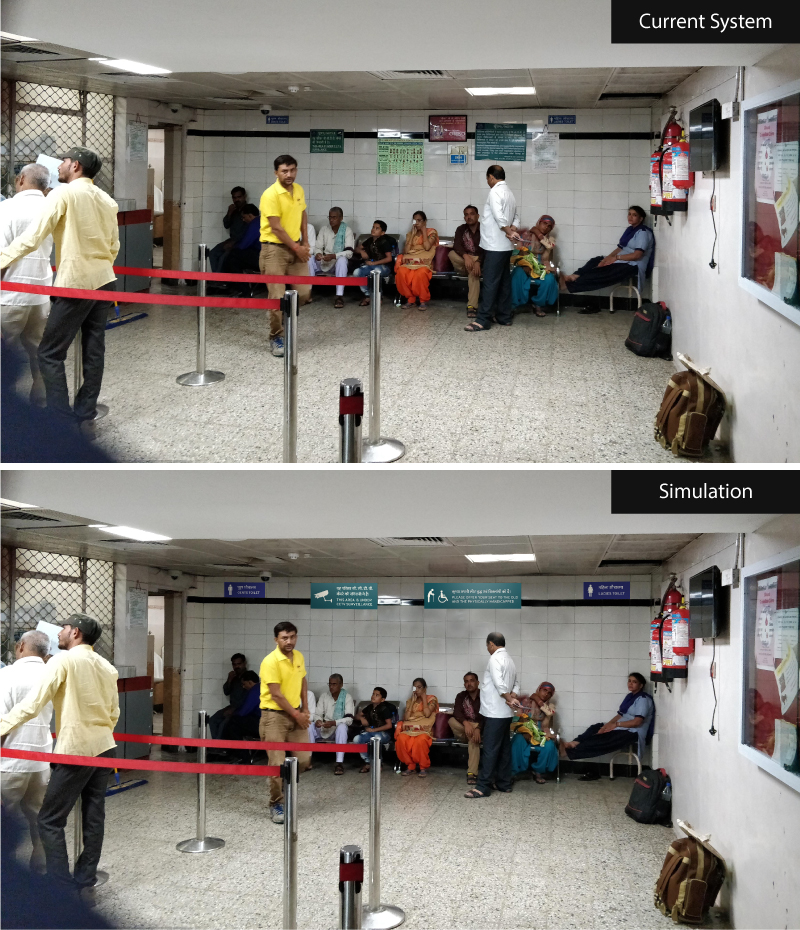
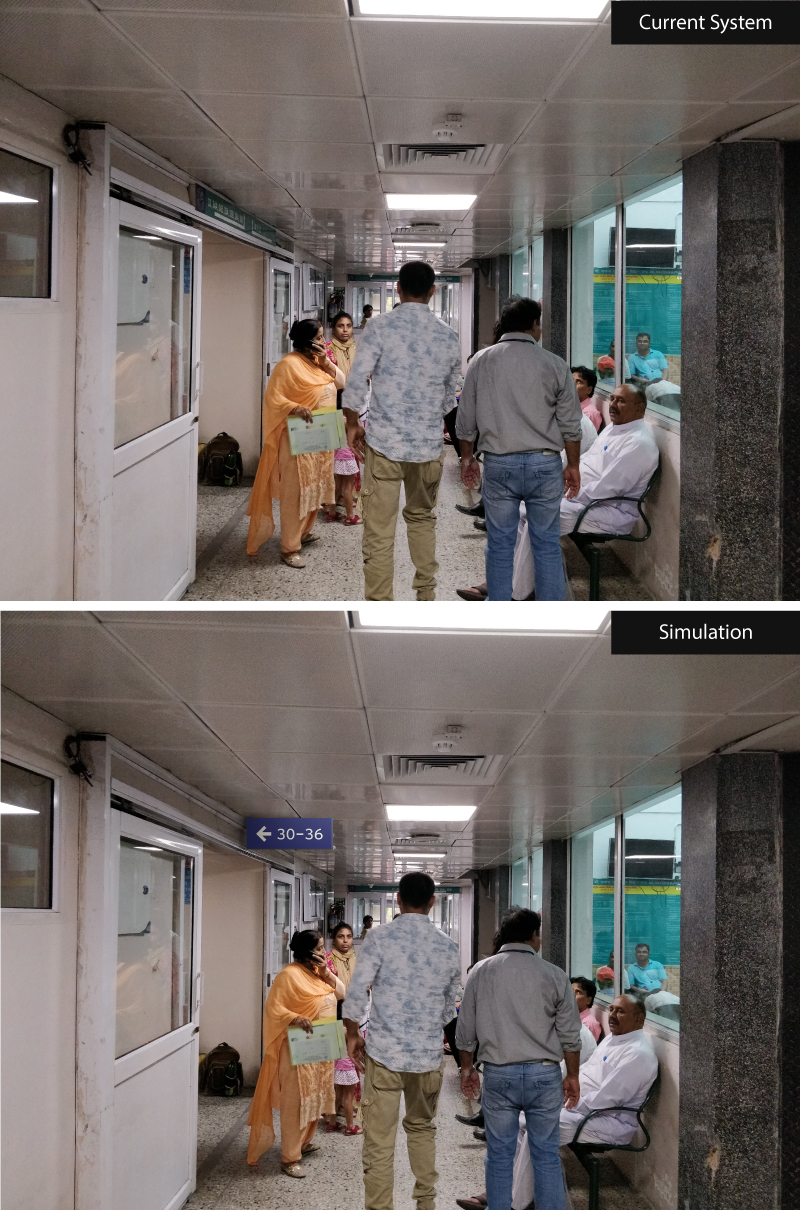
The signages were then digitally simulated at the Centre using Photoshop and presented as a first round of design interventions to the staff and management at the centre. The signages were of two types; wayfinding signages and information signages, differentiated by colour while maintaining the same contrast ratios. Having received positive feedback on the designs, we proceeded with physical prototyping and onsite testing.
Implementation
The signages were successfully implemented at the centre in the following months, and ex-post testing indicated that patients felt more reassured by seeing the signages with clear indications of the route and destination. The broader problem of crowd management and limited space for visitors continues to be an infrastructural problem for which the Centre envisions investing in a major infrastructural overhaul. The next phase of the project involving digital interventions was conducted through Inclunav Maps and Inclunav Routes.